

School Nurses: Still in Short Supply, But Earning Their Keep

A program to add more registered nurses in Massachusetts public schools more than justified its costs by reducing medical costs and the need for parents to stay home from work, according to a new study published in JAMA Pediatrics.
CDC researchers found that $2.20 was saved for each dollar invested in the school nurse program.
The study appears at a time when school districts nationwide have been cutting back on nurses rather than adding them.
In addition, a recent report commissioned by the Lucile Packard Foundation for Children’s Health found that health services for California students with special health care needs vary greatly by school district, are provided by a variety of school staff, operate under a confusing patchwork of regulations, and are often underfunded.
In California, there is one full-time equivalent nurse for every 2,815 students, well above the CDC-recommended ratio of one nurse for every 750 students. In one county, only one nurse serves more than 13,000 students.
See more data on school nurses in California:
Number of School Nurses, By County
Ratio of Students to School Nurses, By County
Related Content:
Cost-Benefit Study of School Nursing Services, JAMA Pediatrics, May 19, 2014
The ‘Hidden Health Care System’ in California Schools and Children with Special Health Care Needs
Posted by Barbara Feder Ostrov
Post Comment
Mental Health Awareness Week: In California, Mental Health Hospitalizations for Children and Youth on the Rise

As National Children’s Mental Health Awareness Week gets under way, we’re highlighting child mental health data available at kidsdata.org:
* Mental health hospitalization rates are rising for teenagers ages 15-19 in California: their mental health hospitalization rate rose 34% between 2007 and 2012.
* In 2012, children and teens faced mental health concerns serious enough to warrant nearly 38,000 hospitalizations.
Nationwide, mental health disorders among children and youth are on the rise, with an estimated one in five American children experiencing problems ranging from mild to life-threatening, according to a 2013 CDC study.
Experts who have studied mental health hospitalizations of children and youth say that while rates of these hospitalizations are higher, in-patient stays are shorter than in previous years possibly due to changes in health insurance authorizations for hospitalization and a decrease in available psychiatric beds.
For a deeper dive into our child mental health data, see these indicators:
Hospitalizations for Mental Health Issues, by Age Group
Depression-Related Feelings, by Grade Level
by Level of Connectedness to School
Number of Youth Suicides, by Age
Self-Inflicted Injury Hospitalizations
Other Resources
National Center for Children in Poverty: Children’s Mental Health
National Institute of Mental Health: Child and Adolescent Mental Health
Social and Emotional Development in Children and Adolescents Knowledge Path
Posted by Barbara Feder Ostrov
Post Comment
Healthy Communities Data Summit: Talking About Big Data and California Communities
![]()
We’re excited to be supporting the Healthy Communities Data Summit on June 11!
The upcoming conference at the University of California-Los Angeles will bring together people working with Big Data to improve health and wellness in California communities.
The Healthy Communities Data Summit is hosted by the Foundation for Healthcare Innovation and Health 2.0, and sponsored by the California HealthCare Foundation, The California Wellness Foundation and the Lucile Packard Foundation for Children’s Health, home to kidsdata.org.
Kidsdata.org’s data manager, Regan Foust, will showcase the site on the panel “New Frontiers for California: Datasets and Resources in Health Care,” which highlights data resources driving the future of public health, new health care startups, and new collaborations.
Here are more highlights from the conference:
- Live demonstrations from new companies and newly captured health data.
- Announcements of state-level projects, case studies, best practices, and lessons learned from access to free government data.
- A full day of high profile panels outlining patient health challenges and needs, as illustrated by timely, relevant health data.
- Publication of new open data challenge efforts and new prize efforts catalyzing citizen innovation efforts & more.
Get more information on the conference, including the agenda and how to register. We look forward to seeing you in Los Angeles on June 11!
Posted by kidsdata.org
Post Comment
By Any Measure, Many California Children Still Live in Poverty
 The percentage of California children living in poverty remains high – even as the nation continues to recover from the recession. Two measures used by the federal government to assess poverty among American families, the Federal Poverty Level and the more state-specific Supplemental Poverty Measure, indicate that a quarter of the state’s children remain in poverty. A third measure suggests the numbers are even higher.
The percentage of California children living in poverty remains high – even as the nation continues to recover from the recession. Two measures used by the federal government to assess poverty among American families, the Federal Poverty Level and the more state-specific Supplemental Poverty Measure, indicate that a quarter of the state’s children remain in poverty. A third measure suggests the numbers are even higher.
The Federal Poverty Level (FPL) for a family of two adults and two children in 2012 was $23,283. Using this standard, about 24% of California children lived in poverty that year, up from about 17% in 2007. The FPL is based on the basic food budget a family needs to meet minimum nutritional requirements but does not take into account other expenses like housing.
To address this limitation, the Census Bureau created the Supplemental Poverty Measure (SPM). Unlike the FPL, the SPM takes into account regional differences in the cost of living (e.g., differences in the cost of food, clothing, shelter, utilities, etc.) and the benefits provided to needy families. According to the SPM, about 27% of California children lived in poverty in 2012, up from 25% in 2009.
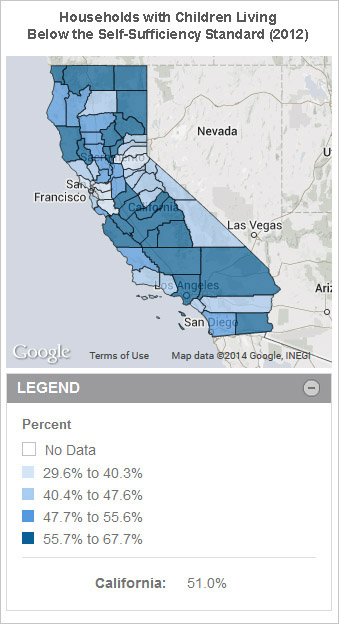
The Supplemental Poverty Measure is only available at the state and national level, however. To assess the local situation, experts created Self-Sufficiency Standards for every California county. These standards calculate the estimated amount of money a family needs to adequately meet all its basic needs without public or private assistance.
On average, these standards are more than double the Federal Poverty Level. For example, the average California Self-Sufficiency Standard for two adults, one preschooler, and one school-aged child is $63,979. Reflecting California’s relatively high cost of living, more than half of families had incomes below the Self-Sufficiency Standard for their county in 2012.
Read more about child poverty in California, including policy implications>>
Posted by kidsdata.org
Post Comment
Data in Your Pocket: Kidsdata.org Goes Mobile
Have you ever been in a meeting and needed quick access to info about kids in California? Good news! Kidsdata.org is now easier to use when you’re on the go: Our data are optimized for mobile devices.

Your smartphone is perfect for looking up fast facts on children’s health and well-being in California. Just navigate to kidsdata.org (you might even want to bookmark it) to find what you’re seeking.
If you have questions about using the mobile version of kidsdata.org, please contact us at [email protected].
RELATED CONTENT:
Tutorial Videos: Get the Most Out of the New Kidsdata.org
ARCHIVED WEBINAR: The New Kidsdata.org: Putting Data to Work for California Children
The New Kidsdata: Using Legislative Maps
Posted by kidsdata.org
Post Comment
National Public Health Week: How California’s Children are Faring

As National Public Health Week gets under way today, it’s a good time to examine how California’s kids are faring on some classic public health measures, including immunizations, exposure to lead and teen birth rates.
Here’s a sampling of public health indicators from kidsdata.org:
IMMUNIZATIONS
California children are required to get several immunizations before entering kindergarten. In 2013, 9 out of 10 California kindergartners received all required immunizations before starting school, but a rise in families using “personal belief exemptions” to avoid some or all required vaccines has public health officials concerned.
See data by county:
Kindergartners with All Required Immunizations
Kindergartners with Immunization Exemptions
LEAD POISONING
Exposure to lead has been linked to lower IQ, behavioral problems and other health problems in children. In 2011, 2,156 children/youth in California ages 0-20 (0.3% of all children tested) were found to have elevated levels of lead in their blood, down from 0.6% in 2007. While elevated blood lead levels are defined as 9.5 micrograms per deciliter or more, most public health officials agree that there is no safe level of exposure to lead. Not all children in the state are tested for lead exposure, however, and the available data may understate lead exposure.
See data by county: Children/Youth with Elevated Blood Lead Levels, by Age
TEEN BIRTHS
In what’s widely regarded as a public health success story, teen births have declined sharply in both California and the U.S., although racial disparities remain. The teen birth rate in California decreased by 59% between 1995 and 2012, from 62.9 to 25.7 per 1,000 young women ages 15-19.
See data by county:
LEARN MORE
Be sure to take a look at these other public health indicators, too!
Air Quality: Annual Average Particulate Matter Concentration
Students Who Are at a Healthy Weight or Underweight, by Grade Level
Breastfeeding of Newborns, by Breastfeeding Status
Children Drinking One or More Sugar-Sweetened Beverages Per Day
Children Who Ate Fast Food Two or More Times in the Past Week, by Age Group
Children Who Eat Five or More Servings of Fruits/Vegetables Daily, by Age Group
Sexually Transmitted Infections
Water Quality Violations, by Violation Type
Infants Whose Mothers Received Prenatal Care in the First Trimester
Posted by Barbara Feder Ostrov
Post Comment
Tutorial Videos: Get the Most Out of the New Kidsdata.org
Kidsdata.org’s updated look and new features make it easier than ever to find and use data about the health and well-being of children. If you’re new to the site, or just need a refresher, here are some (short!) video tutorials on how to get the most out of kidsdata.org. Each runs less than three minutes, so you’ll be able to learn new skills fast.
Kidsdata.org Overview: Learn the basics of what kidsdata offers and how to navigate the site.
Finding Data by Topic: Discover several techniques to search for data about topics ranging from physical health to educational achievement to emotional well-being.
Finding Data by Region and Demographic Group: Explore how to find data by county, school district, city, legislative district, age range, racial and ethnic categories, and more.
Customizing Data: Find out how to create data visualizations including trend charts, bar graphs and maps, and tailor them to meet your needs.
Downloading and Sharing Data: See various ways to download large data sets, share data visualizations through social media, and embed charts and graphs on your website or in your blog post.
Having Trouble Finding What You’re Looking For? Learn how use search features and navigation menus to find the data you need.
E-alerts and Kidsdata Newsletter: Check out how to sign up for data alerts tailored to your interests, along with our newsletter.
Questions? Contact us at [email protected] or see our Help page.
Posted by Barbara Feder Ostrov
Post Comment
New Study: The ‘Hidden Health Care System’ in California Schools and Children with Special Health Care Needs

The recent controversy over who is permitted to administer diabetes injections to children in school underscores a larger issue: Health services for California students with special health care needs vary greatly by school district, are provided by a variety of school staff, operate under a confusing patchwork of regulations, and are often underfunded, according to a new study.
See preliminary findings from the study>>
Researchers from California State University-Sacramento’s School of Nursing analyzed 2011-2012 state education data, interviewed school education experts, and conducted a large-scale survey of certified school nurses who are members of the California School Nurses Association. The research, which will be presented today at the California School Nurses Association conference in Sacramento, was funded by the Lucile Packard Foundation for Children’s Health.
California is home to an estimated 1.4 million children with chronic health issues, ranging from mild to life-threatening. About 16% of 6-to-11 year-olds and 20% of 12-to-17 year-olds have a special health care need that may require additional health services at school to allow for their full participation.
Among the study’s findings:
- 57% of California public school districts report having no school nurse personnel. These districts serve about 1.2 million students, about 20 percent of all public school students in the state.
- School nurse responsibilities have become more complex, including inserting urinary catheters, helping children with their feeding tubes, changing ostomy bags, monitoring oxygen tubes, testing blood sugar, and administering anti-seizure medication.
- Unlicensed school staffers provide sometimes complex medical care in the absence of school nurses. While many staffers are trained by nurses, there is little statewide regulation or monitoring of their training.
- Children with special health care needs aren’t always identified by school staff and may not receive services that could help them stay and succeed in school.
“California has very weak requirements governing school health and provides little data or guidance for school nurses and administrators to manage the care of children with special health care needs,” said the study’s lead author Dian Baker, a pediatric nurse practitioner and associate professor of nursing at CSU-Sacramento. “We can do better.”
See student-to-school nurse ratios by county>>
California has the largest population of children with special health care needs of any state. The federal Education for All Handicapped Children Act (1975), as amended in the Individuals with Disabilities Act (2004), was designed to ensure that children with disabilities have the opportunity to receive a free appropriate public education.
The study’s authors recommend several statewide policies and local practices that could help improve the hidden health system in California schools, not just for children with special health care needs, but for all students.
- Require systematic data collection and reporting systems in school districts to identify and serve children with special health care needs, and to monitor their health and educational outcomes.
- Require that all personnel delivering health services in schools receive mandatory training, including first aid, CPR and procedures needed to serve specific children in each school.
- Require that funds generated through Medi-Cal Administrative Claiming be earmarked to support school health services in the same manner as are Local Education Agency funds.
Posted by Barbara Feder Ostrov
Post Comment
ARCHIVED WEBINAR: The New Kidsdata.org: Putting Data to Work for California Children
If you missed our February webinar on how to use kidsdata.org after our recent redesign, the recording is now available!
The webinar covers how to find the data you need, tailor the data format for your needs, export data for analysis, and communicate your data in reports, presentations, proposals, social media and more.
Questions? Email us at [email protected]. To sign up for announcements of upcoming webinars, data alerts and other news from kidsdata.org, click here.
Posted by kidsdata.org
Post Comment
Updated AAP Policy on Retail Clinics: A Wake Up Call for Pediatricians

The American Academy of Pediatrics’ recently updated policy statement opposing retail clinics for children’s health care drew a surprising amount of attention this week.
While the AAP characterized the clinics as providing fragmented care at odds with the ideals of coordinated care and the medical home, some observers saw the statement as an effort by pediatricians to protect their turf. The AAP has long opposed the rise of retail clinics, which are open late, don’t require appointments and post their prices up front.
In an editorial published in JAMA Pediatrics last year, Dr. Edward Schor, senior vice president of the Lucile Packard Foundation for Children’s Health, urged his fellow pediatricians to embrace some of the customer-focused practices that have made retail clinics so successful.
To improve the care experience for busy families, pediatricians who haven’t already done so should consider expanded office hours and after-hours care, same-day and walk-in appointments, co-location of frequently used services, and transparent pricing, Schor noted.
“Families are sending a clear message to pediatric practices through their use of RBCs (retail-based clinics). Although they appreciate the array of services available from their pediatrician, they value convenience and low cost and see no apparent difference between a pediatric practice and an RBC in quality of care for minor illnesses,” Schor wrote.
Related Content
Docs Oppose Retail-Based Clinics For Kids’ Care, USA Today
AAP Principles Concerning Retail-Based Clinics
Medical Home: What’s in a Name?
Toward a “Triple Aim Medical Home” for Children with Special Health Care Needs
Aiming for Change: Achieving Triple Aim Goals in Pediatricians’ Practices
Posted by Barbara Feder Ostrov
Post Comment