

Quick Tip: Data Overview Guide
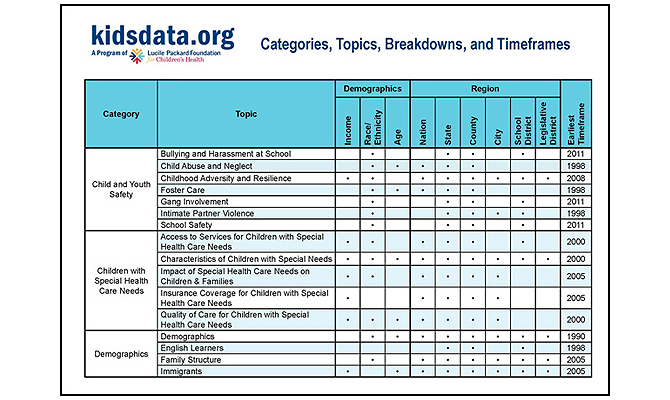
Our Data Overview Guide provides a complete list of all the topics available on kidsdata.org. You can quickly view popular data breakdowns for each topic from demographics like income, race/ethnicity and age to regions, including national, state, county, city, school district and legislative district. Also, see the earliest timeframe available for the topic to assess change over time.
Get more information like this overview by visiting kidsdata.org/about.
Posted by kidsdata.org
Post Comment
School Climate and Children’s Health
Students with Low Levels of School Connectedness, by Race/Ethnicity, 2013-2015
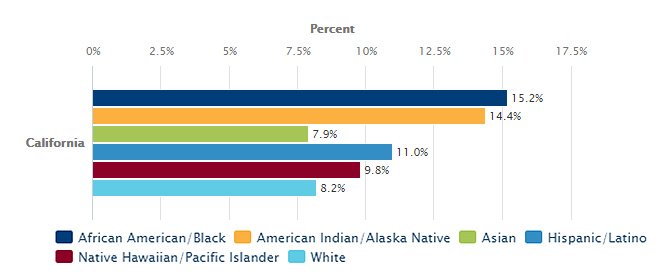
A positive school climate is an important factor that defines effective schools. When school climate is positive, students are more likely to succeed academically and engage in healthy behaviors. A key measure of school climate is level of school connectedness, which takes into account if students feel happy, safe, close to people, and a part of school, and that teachers treat them fairly.
Improving school climate is a promising strategy to narrow achievement gaps among groups of students. However, student groups experience school climate differently. For example, in California, higher percentages of African American/Black and American Indian/Alaskan Native students report low levels of school connectedness in 2013-2015 (15% and 14%, respectively) compared with Asian and White students (both 8%). In addition to race/ethnicity, gaps also exist by parent education level and sexual orientation. By creating an inclusive, safe, and academically challenging school climate and utilizing targeted interventions for some groups, we can expect improved academic and health outcomes for all students.
California law now requires school districts to address school climate as part of the Local Control and Accountability Plans. Learn more about policy and practice recommendations to nurture a strong school climate.
This data release is a part of Kidsdata’s Youth in Schools series. In partnership with WestEd, we are featuring data from the California Department of Education’s California Healthy Kids Survey.
Data in Action
See Kidsdata at the Positive Behavioral Interventions and Supports (PBIS) conference in Sacramento on September 25th where we will discuss identifying inequity to target interventions.
Recently Released Data
We are continuously updating our data. Click the links below to see the latest:
Posted by kidsdata.org
Post Comment
Youth in Schools Data Available on Kidsdata

A comprehensive suite of data, Youth in Schools, includes new and updated indicators across more than a dozen topics from the viewpoint of California’s students and school staff. These data are available for state, county, and school district levels, and student-reported data are easily customizable by grade level, gender, race/ethnicity, sexual orientation, parent education level and level of school connectedness.
Youth in Schools data come from the California Healthy Kids Survey (CHKS) and California School Staff Survey (CSSS), the largest statewide surveys of school climate, risk behaviors, and protective factors in the nation. This data release is made possible by a partnership with WestEd who developed and administered these surveys for the California Department of Education.
Explore behaviors, identify disparities, and take action with hundreds of findings about Youth in Schools at your fingertips.
A complete list of Youth in Schools data is below. Learn more about the data, including helpful webinars, in our A Deeper Look section.
List of Youth in Schools Data
Access to Services for Children with Special Needs
Bullying and Harassment at School
- Bullying/Harassment
- Bias-Related Bullying/Harassment
- Disability as Reason for Bullying/Harassment
- Gender as Reason for Bullying/Harassment
- Race/Ethnicity or National Origin as Reason for Bullying/Harassment
- Religion as Reason for Bullying/Harassment
- Sexual Orientation as Reason for Bullying/Harassment
- Cyberbullying
- Student Bullying/Harassment Is a Problem at School (Staff Reported)
Children’s Emotional Health
- Depression-Related Feelings
- Students Who Are Well-Behaved (Staff Reported)
- Student Depression or Mental Health Is a Problem at School (Staff Reported)
- School Emphasizes Helping Students with Emotional and Behavioral Problems (Staff Reported)
Demographics
Family Structure
Gang Involvement
Health Care
Nutrition
Physical Fitness
- Physical Education and Activity Opportunities at School (Staff Reported)
- Students Who Are Healthy and Physically Fit (Staff Reported)
Pupil Support Services
- School Provides Adequate Counseling and Support Services for Students (Staff Reported)
- School Provides Services for Substance Abuse or Other Problems (Staff Reported)
- School Collaborates with Community Organizations to Address Youth Problems (Staff Reported)
School Attendance and Discipline
- Reasons for School Absence in Past Month
- Truancy (Student Reported)
- Truancy or Cutting Class Is a Problem at School (Staff Reported)
School Climate
- Academic Motivation (Student Reported)
- School Connectedness (Student Reported)
- School Supports (Student Reported)
- Caring Relationships with Adults at School (Student Reported)
- High Expectations from Adults at School (Student Reported)
- Meaningful Participation at School (Student Reported)
- Students Who Are Motivated to Learn (Staff Reported)
- School Motivates Students to Learn (Staff Reported)
- School Is a Supportive and Inviting Place to Learn (Staff Reported)
- Adults at School Care About Students (Staff Reported)
- Adults at School Believe in Student Success (Staff Reported)
- School Welcomes and Facilitates Parent Involvement (Staff Reported)
- School Gives Students Opportunities to Make a Difference (Staff Reported)
- School Fosters Youth Resilience or Asset Promotion (Staff Reported)
- Students Respect Each Other’s Differences (Staff Reported)
- Cultural or Racial/Ethnic Tension at School (Staff Reported)
School Safety
- Perceptions of School Safety
- Fear of Being Beaten Up at School
- Physical Fighting at School
- Carrying a Gun at School
- Carrying a Weapon Other Than a Gun at School
- Perceptions of School Safety for Students (Staff Reported)
- Perceptions of School Safety for Staff (Staff Reported)
- Student Physical Fighting Is a Problem at School (Staff Reported)
- Student Weapons Possession Is a Problem at School (Staff Reported)
Youth Alcohol, Tobacco, and Other Drug Use
- Alcohol/Drug Use in Past Month
- Alcohol/Drug Use on School Property in Past Month
- Alcohol Use in Past Month
- Alcohol Use in Lifetime
- Binge Drinking in Past Month
- Drinking and Driving or Riding with a Driver Who Has Been Drinking
- Cigarette Use in Past Month
- Cigarette Use in Lifetime
- E-Cigarette Use in Past Month
- E-Cigarette Use in Lifetime
- Marijuana Use in Past Month
- Marijuana Use in Lifetime
- Student Alcohol and Drug Use Is a Problem at School (Staff Reported)
- Substance Abuse Prevention Is an Important Goal at School (Staff Reported)
- Substance Use Prevention Education Is Provided at School (Staff Reported)
Youth Suicide and Self-Inflicted Injury
A Deeper Look
Issue Briefing: School Climate and California LGB Youth
Click the image to view the recording and slides:
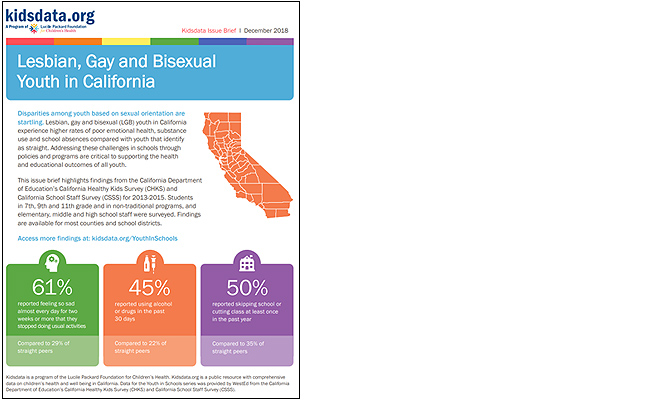
Issue Brief: Lesbian, Gay and Bisexual Youth in California
Click image to view brief:
Data Briefing: New Data on Youth in Schools
Data Briefing Recording:
Posted by kidsdata.org
Post Comment
Children of Immigrant Families
Children Living with One or More Foreign-Born Parent, 2016
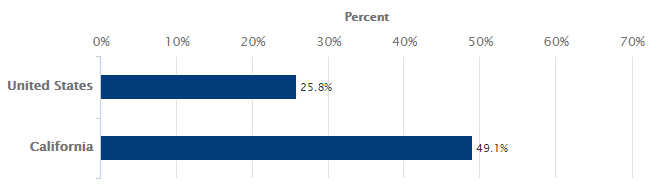
Federal immigration policies and rumors about impending policies have a bigger impact on children in California than on children in most other states. In California, nearly half of children have at least one foreign-born parent. In contrast, this group accounted for about one-quarter of all children in the United States. In California, odds are youth sense the rising fear and uncertainty of family stability at home or in their community, which over time can have negative impacts on emotional and physical health.
The direction of current immigration policy may have unintended consequences beyond harming child health and well being. Without immigrant parents, the United States would have about one-million fewer children (PDF, pg. 10), adding to an already documented shortage of children relative to adults. Fewer children means increasingly serious consequences for supporting the future labor force and sustaining an aging population. Each child — regardless of country of origin — is more important to our future than ever before. The health and well being of all children should be our nation’s priority.
Data in Action
Children’s Partnership and the California Immigrant Policy Center share research findings and identify actions to support healthy development of children in immigrant families in The Effect of Hostile Immigration Policies on Children’s Mental Health.
Recently Released Data
We are continuously updating our data. Click the links below to see the latest:
- Children Living in Limited English-Speaking Households (65,000 Residents or More)
- Children Living with Foreign-Born Parents (65,000 Residents or More)
- Children Living with Foreign-Born Parents, by Income Level (65,000 Residents or More)
- Foreign-Born Population, by Age Group (65,000 Residents or More)
Posted by kidsdata.org
Post Comment
Maternal Emotional Health Topic New to Kidsdata
Kidsdata and the California Department of Public Health (CDPH) have partnered to share important new measures of maternal mental health before and after a live birth from the Maternal and Infant Health Assessment (MIHA) survey. A woman’s emotional well-being during this time is central to her health and to her infant’s development. Depression during and after pregnancy is a serious medical condition that requires culturally appropriate and trauma-informed support and treatment.
Guest authors, Christine Rinki and Amina Foda, Research Scientists with the California Department of Public Health, share important findings about symptoms of depression among women who recently gave birth in California:
Symptoms of depression during and after pregnancy
According to a recent Data Brief (PDF) from the California Department of Public Health’s Maternal and Infant Health Assessment (MIHA) survey, about one in five women who give birth in California experience symptoms of depression during or after their pregnancy.
Although relatively minor changes in mood the first few days after childbirth are common, depression that arises during or after pregnancy is a mood disorder characterized by intense feelings of sadness, anxiety or despair that last for two weeks or longer and prevent women from doing their daily tasks.
If untreated, depression during or after pregnancy increases the risk of cognitive and emotional development problems in infants, and may result in fundamental changes in the brain that can have lasting effects into childhood. Depression occurring after the baby is born can negatively impact women’s breastfeeding practices and ability to bond with their infants. Importantly, depression at any point during or after pregnancy increases the risk that women could develop chronic depression or die by suicide once the baby is born, which in turn have profound impacts on children.
Thankfully, with the appropriate care, most women can experience full recovery. Best practices to address maternal mental health include screening for depression throughout prenatal and postpartum care, and increasing the availability of services that are affordable, culturally and linguistically appropriate, and that acknowledge the history of trauma common among women with depression.
Prenatal and postpartum symptoms of depression in California
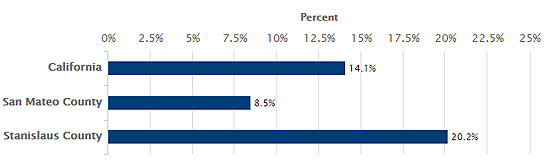
In California, 14.1% of women experienced prenatal symptoms of depression and 13.5% experienced postpartum symptoms of depression. Many, but not all, women who experienced symptoms of depression would be diagnosed with clinical depression.
There was substantial geographic variation among counties with data. Prenatal symptoms of depression ranged from 8.5% in San Mateo County to 20.2% in Stanislaus County, while postpartum symptoms of depression were 9.8% in Yolo County and 18.8% in San Joaquin County.
Prenatal Symptoms of Depression
Prenatal symptoms of depression: Important, but often overlooked
Despite the serious risks associated with prenatal depression, including low birth weight, premature delivery and changes in infant brain development, its importance is often overlooked. MIHA results (PDF) indicate that prenatal symptoms of depression often precede postpartum symptoms of depression in women. In California, 53% of the women who experienced prenatal symptoms of depression went on to report them in the postpartum period. In contrast, only 7% of women without symptoms of depression during pregnancy experienced them after pregnancy. In order to have the best chance of improving outcomes for the mother and infant, routine screening and treatment for depression should begin early in pregnancy, a time when women have increased contact with the health care system.
Disparities in prenatal symptoms of depression
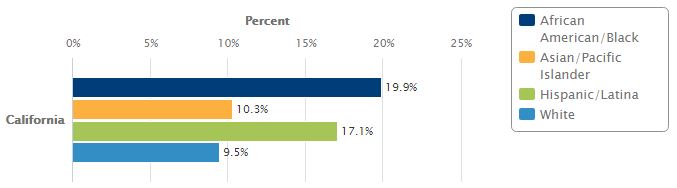
Though symptoms of depression during and after pregnancy can affect women regardless of their background or circumstances, some groups in California experience them at disproportionately high levels. Women who are Black or Latina had higher rates of symptoms of depression compared to other racial or ethnic groups. During pregnancy, symptoms of depression were twice as common for Black (19.9%) and Latina (17.1%) women compared to White (9.5%) and Asian/Pacific Islander (10.3%) women. Reports of prenatal and postpartum symptoms of depression were highest among women with incomes below poverty (20.7% and 18.2%, respectively), and declined as income increased.
Prenatal Symptoms of Depression by Race/Ethnicity
Programs that address perinatal emotional and mental health
The Maternal, Child and Adolescent Health Division of the California Department of Public Health strives to improve maternal emotional and mental health by tailoring primary prevention to address the social factors that lead to poor emotional and mental health and to promote individual protective factors. Additionally, many MCAH Division programs screen for symptoms of depression using validated tools, and provide appropriate referrals and support for women in need of care. For example, the Black Infant Health Program conducts group sessions with complementary case management that provide social support while helping women develop skills to reduce stress, enhance emotional well-being and develop life skills in a culturally affirming environment that honors the unique history of Black women. The California Home Visiting Program funds home visiting models throughout the state that use a strengths-based approach to enhance the mother-baby relationship. Home visitors address family needs such as financial struggles, relationships, and navigating the health care system, while support groups and mental health consultation directly address emotional well-being.
Striving for equity in perinatal emotional and mental health
The underlying causes of the maternal mental health disparities identified in the MIHA Data Brief are multifaceted. For example, Black and Latina women in California experience higher levels of risk factors for depression such as poverty and childhood hardships compared to other racial and ethnic groups. Institutional racism (the practices of social and political institutions that result in unfair treatment of Black, Latina and other minority groups) likely plays a role in explaining the concentration of risk factors, and the subsequent racial and ethnic disparities in depressive symptoms. Achievement of emotional and mental well-being for all California women during and after their pregnancies can have profound societal impacts. Action to address social factors can improve outcomes for low-income and minority families.
Recently Released Data
We are continuously updating our data. Click the links below to see the latest:
Posted by kidsdata.org
Post Comment
Access to High Quality Health Care for California Children
Guest author, Holly Henry, PhD, is a Program Officer at the Lucile Packard Foundation for Children’s Health. She works to improve the system of care for children with special health care needs. Dr. Henry focuses on promoting effective care coordination, a practice that links children and their families with appropriate services and resources to support optimal health.
Every child deserves high quality health care that is accessible, family-centered, culturally competent, coordinated, continuous, compassionate, and comprehensive. Unfortunately, our current system of care for children is deeply fragmented and health needs are not being met. One approach to strengthening coordination of care is providing care through a medical home. The medical home recognizes the family as a constant in a child’s life and emphasizes partnership between health care professionals and families. It facilitates collaboration between patients, clinicians, medical staff, and families. More importantly, a medical home extends beyond the four walls of a clinical practice – it includes specialty care, educational services, and family support.
Receipt of Care Within a Medical Home, 2016
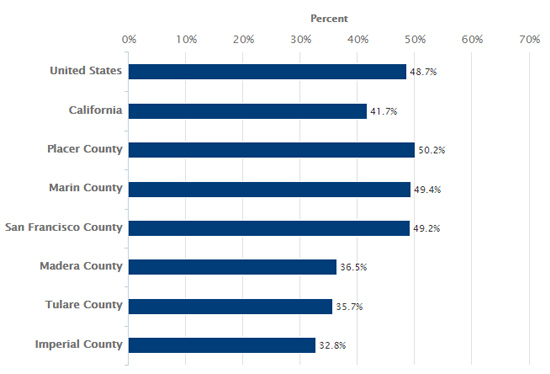
In 2016, 42% of California children received care within a medical home compared with 49% of children nationally. Receipt of care within a medical home varies across the state. The counties with the highest and lowest percentages of children receiving care within a medical home, among counties with data, are also noted in the graph above.
Children receiving care from a medical home have fewer outpatient visits and families report better child health status. Families also report increased satisfaction with their child’s care. For children with special health care needs this can also mean decreased length and frequency of hospitalizations and lower out-of-pocket spending.
All children would benefit from being cared for within a medical home. See how your county is faring.
Data in Action
Learn more about care coordination and how it can help reduce health care fragmentation. The Lucile Packard Foundation is hosting a webinar on care coordination for children with medical complexity on July 26 at 10 am PST. Audience Q&A is highly encouraged. Attendees can listen via web or phone. Learn more and register.
Recently Released Data
School Provides Services for Students with Special Needs (Staff Reported) [NEW]
Posted by kidsdata.org
Post Comment
Childhood Adversity Data Available by County, City and School District
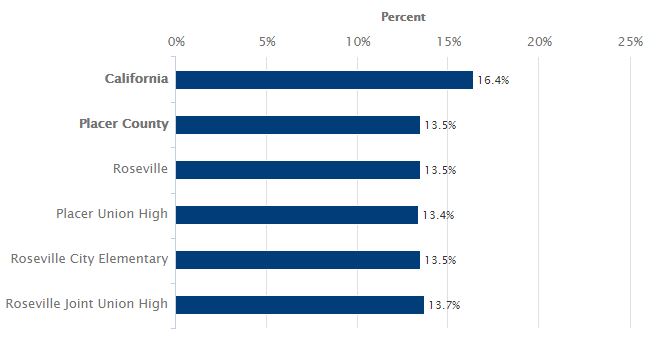
Children with Two or More Adverse Experiences (Parent Reported), 2016
ACEs by County
Adverse childhood experiences – such as family separation, abuse, exposure to violence, and poverty – can have negative, long-term impacts on the health and well being of a child. According to the American Academy of Pediatrics, separating children from their parents, for example, removes the buffer of a supportive adult or caregiver who can help mitigate stress and protect against chronic conditions like depression, post-traumatic stress disorder, and heart disease. The more intense, repetitive and long-lasting the events experienced, the greater and more sustained their impact.
Childhood adversity data based on parent responses about their child’s experiences are available on Kidsdata.org. The data come from the 2016 National Survey of Children’s Health, and cover many California counties, cities and school districts. For example, Placer County, which has among the lowest rates of childhood adversity in the state, can be explored further by looking at Roseville, a city within the county, or by school districts within the county. See what childhood adversity data are available in your local area by clicking the + icon next to the county name.
Data in Action
Consider attending the 2018 ACEs Conference & Pediatric Symposium: Action to Access, October 15-17 in San Francisco. The conference explores problems of access, and how to reduce children’s exposure to adversity and its traumatic effects. It is co-hosted by the Center for Youth Wellness and ACEs Connection.
Join a community of advocates and practitioners committed to reducing childhood adversity and increasing resilience, visit acesconnection.org.
Posted by kidsdata.org
Post Comment
The Mental Health Journey of a Mother and Daughter
Recently Released Data
We are continuously updating our data. Click the links below to see the latest:
Health Insurance Coverage (Regions of 65,000 Residents or More), by Age Group
Health Insurance Coverage (Regions of 10,000 Residents or More), by Age Group
Receipt of Care Within a Medical Home (Regions of 65,000 Residents or More) [NEW]
School Provides Adequate Health Services (Staff Reported)
Posted by kidsdata.org
Post Comment
Three Mental Health Bills for California Children
Posted by kidsdata.org
Post Comment
How to View Data by School District

Data in Action
The Kidsdata team will be at the California School-Based Health Conference on Friday, May 18, in Sacramento, CA. The event brings together providers, educators, advocates, and other leaders in the school-based health care movement across the state. Be sure to stop by our booth to say hello!
Posted by kidsdata.org
Post Comment