Compelling data go beyond just the numbers. Did you know that all 600+ indicators on Kidsdata include definitions, data sources, and notes?
Click on the “Definition, Source & Notes” link on the indicator page:

You’ll find information to help you interpret the data:

Check out more helpful tips »
Posted by kidsdata.org
Post Comment
Children Ages 0-5 with Elevated Blood Lead Levels, 2013

Lead is a leading environmental threat to children’s health in the U.S. When children are exposed to lead—usually through contaminated dust, paint, or soil—it can have lifelong adverse effects, such as disrupted postnatal growth, hearing and learning disabilities, lowered IQ scores, behavioral problems, difficulty paying attention, and hyperactivity.
More than 1,200 California children ages 0-5 who were tested in 2013 had blood lead levels at or above 9.5 micrograms per deciliter (μg/dL), well over the CDC reference level of 5μg/dL. Experts agree that prevention is the best course of action. While regulations and abatement efforts have helped reduce the prevalence of lead in the environment in recent decades, lead continues to pose a health and behavioral threat to children. More must be done.
See policy options that could make a difference »
From October 22 to 28, the CDC and U.S. Department of Health and Human Services are promoting National Lead Poisoning Prevention Week.
Posted by kidsdata.org
Post Comment
Massive demographic changes create challenges, elevate economic role of next generation
Ensuring children’s health and well being in the U.S. has never been more critical to the nation’s economic and political future, according to The New Importance of Children, a report co-funded by the Lucile Packard Foundation for Children’s Health and the Children’s Hospital Association.
The Baby Boomer generation is aging and retiring at the same time that birth rates are declining, altering the social and economic landscape. This disproportion due to the relative shortage of children makes each child—regardless of gender, ethnicity, geographic residence or economic background—more important to our future than ever before. As advocates we need to champion the priority of children to those who have the power to promote change.
Read the latest findings »
Posted by kidsdata.org
Post Comment
San Diego, Ventura, Riverside, and Los Angeles Counties saw some of the biggest declines from 1980 to 2016. However, San Bernardino had the most days for 2016 with 106 days above the regulatory standard.
Ozone is a serious environmental threat to children’s health and is linked to abnormal lung development as well as asthma and other lung diseases. Strengthening laws and regulations that limit harmful emissions from vehicles, power plants, refineries, and other sources of air pollution is crucial.
See your county’s progress »
Posted by kidsdata.org
Post Comment
“Our group presented your data to our county health managers and supervisors, and it provided the credibility and detailed info we needed to get some action.” – survey respondent
A warm thank-you to all who contributed to our survey. We loved learning about how members of the Kidsdata community, from program staff and county administrators to advocates and educators, are using data to take action.
Top Ways Kidsdata Is Driving Action
We are inspired by the ways you are using Kidsdata to ensure that all children are able to reach their maximum health potential. Check out the top ways Kidsdata is driving action:
1. Supporting the need for programs and initiatives through grant proposals
2. Promoting the importance of children’s health in presentations, research projects, and reports
3. Setting strategic goals and evaluating programmatic outcomes
Kidsdata aims to be a leading resource for those who work on behalf of children in California—that’s you!
Please continue to share how Kidsdata has made a difference for you. If you have additional suggestions on how Kidsdata can support your work, please contact us at [email protected].
Posted by kidsdata.org
Post Comment
Kidsdata is excited to introduce its newest topic, Health Status. Check out self- and parent-reported data on whether a child’s health status is fair/poor, good, or excellent/very good. The data are available overall, by race/ethnicity, and by family income level for California and for counties.
Health status during childhood sets young people on a path toward good or poor health in adulthood. In California, children’s health status has improved overall and for each race/ethnicity for which we have data since 2001. Most notably, 68 percent of Hispanic/Latino children were in excellent or very good health in 2013-2014 compared with 55 percent in 2001. In addition, the gaps between racial/ethnic groups narrowed during this time period.
Explore our new topic »
Policy Implications
Healthy young people tend to become healthier and more educated adults who are better able to contribute to society than those who struggle with health problems, which means a stronger workforce and reduced strain on public service systems. Nurturing California’s children today may improve the state’s future social and economic well being.
Efforts to improve children’s health can be strengthened by recognizing the wide range of influences on children’s lives including social, economic, environmental, biological, and behavioral influences. Policies and programs that could improve children’s health include implementing cross-sector strategies that go beyond traditional health care and ensuring that every child has access to family-centered, culturally-competent, and coordinated health care within a “medical home.”
See additional policy implications »
We still need your input!
The Kidsdata team is devoted to providing the evidence you need to improve children’s health and well being. Tell us how we can better support your work! Complete a brief survey by September 1 and enter to win a $50 Amazon gift card.
Take the survey »
Posted by kidsdata.org
Post Comment

The Lucile Packard Foundation for Children’s Health is pleased to welcome Alice Chiang, senior manager of communications and external relations, to the Kidsdata team. Alice is passionate about promoting communities of health for children. Prior to joining the Foundation, she was the communications manager for an organization in New York City focused on improving school food and healthy food access. As a Bay Area native, she is excited to be back in her home state and help make health care systems change for children across California.
Alice received her undergraduate degree in molecular and cell biology from University of California, Berkeley, and her master’s degree in food studies from New York University. Alice can be reached by email.
We still need your input!
The Kidsdata team is devoted to providing the evidence you need to improve children’s health and well being. Tell us how we can better support your work! Complete a brief survey by September 1 and enter to win a $50 Amazon gift card.
Take the survey »
Posted by kidsdata.org
Post Comment
The Kidsdata team is devoted to providing the evidence you need to improve children’s health and well being. How can we better support your work? What would make the site more useful to you? Now’s your chance to tell us!
Please share your thoughts in a brief survey. In about 10 minutes, you can help shape the future of Kidsdata. The survey will close September 1.
After completing the survey, you can enter a drawing to win one of five $50 Amazon gift cards. You will also have the opportunity to join the inaugural Kidsdata Super User Group, whose members will provide additional feedback on proposed Kidsdata features.
Thank you for your input!
Take the survey »
Posted by kidsdata.org
Post Comment

Disconnected youth—teens who are neither enrolled in school nor working—may be more likely than their peers to experience poor health, lower incomes, and unemployment as adults. They are also more likely to become involved in illegal activity and become dependent on public aid. In 2013, disconnected youth cost U.S. taxpayers an estimated $27 billion in costs related to incarceration, public assistance, lost tax revenues, and lost earnings.
In 2011-2015, eight percent of California teens ages 16-19 were neither in school nor working. The percentage of disconnected youth in counties ranged from a low of three percent in Yolo County to a high of 14 percent in Mendocino County.
Trends in the rates of disconnected youth varied among counties, cities, school districts, and legislative districts, while the statewide trend saw little change.
Learn more »
Cities Re-Connecting Their Youth
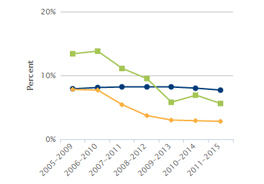
Daly City and Madera are among cities that have seen substantial improvement in re-engaging their youth since 2005-2009. Daly City has improved by five percentage points and Madera has improved by eight percentage points, both dropping below the California state average.
Learn more »
Cities with Increasing Rates of Disconnected Youth
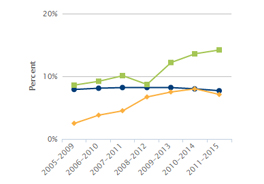
West Covina and Yuba City are among cities that have seen an increase in percentages of disconnected youth since 2005-2009. West Covina has increased by five percentage points and Yuba City has increased by six percentage points, both near or above the California state average.
Learn more »
Policy Implications
Policy solutions range from those that prevent youth from becoming disconnected in the first place to those that re-engage disconnected youth with school and work.
Since teen engagement is related to early school achievement and positive early learning experiences, effective solutions include home-visiting programs for struggling families, quality preschool, and safe and supportive K-12 schools to ensure children have access to quality education and stable, caring environments. To engage older youth, their participation in youth advisory councils, volunteer or community projects, and service learning allows them to become active decision-makers, take on leadership roles, and contribute to the community. Help in creating such opportunities can come from improved statewide coordination and cross-sector community collaboration, both of which can foster integrated approaches to support at-risk and disconnected youth.
See additional policy implications »
Posted by kidsdata.org
Post Comment
 by Edward Schor, MD, Senior Vice President at the Lucile Packard Foundation for Children’s Health
by Edward Schor, MD, Senior Vice President at the Lucile Packard Foundation for Children’s Health
The importance of social factors in determining individuals’ health status and their use of health care services has been receiving increasing attention. A recent report from the Bipartisan Policy Center suggests that opportunities to control health care costs reside primarily in addressing patients’ social and behavioral care needs. The report lays out the arguments for integrating social and medical services and, ideally, their funding, to better serve vulnerable patients with complex care needs.
To date, most of the experimentation within the health care system to address underlying social determinants of health has occurred within the framework offered by Medicare. Such interventions have focused on home-based, patient-centered care, supportive housing, in-home meal delivery, and community-based assistive services. They have yielded improvements in the health of the individuals served and some reductions of health care use. Some states have used Medicaid waivers to allow provision of certain community-based services. Within child health there have been experiments offering similar service options, such as intensive, comprehensive case management to patients and families, housing assistance, and referral for social and legal services.
With a very few, notable exceptions, all of these early efforts to address social determinants of health were built on a medical model, i.e., identifying and treating specific factors contributing to the individual’s poor health. Our existing service delivery systems, which are designed to hew to this traditional model, have had some success but at unsustainable costs.
A public health approach to better serve populations as opposed to individuals would be more efficient and effective. Implementing broad changes in social programs can reduce potentially adverse circumstances that contribute to poor health and harmful health behaviors. Fee-for-service payment schemes perpetuate an individual-based approach to solving health problems. Adopting a capitated model in which all costs are covered by a single advance payment, such as those used by accountable care organizations, can encourage but does not necessarily assure that population-based, integrated approaches will be adopted.
Some health care systems, guided by their own cost-benefit analyses, are addressing social determinants of health, not as their mission but rather as cost-saving strategies for individual or targeted groups of high-risk patients, under the rubric of value-based purchasing. This is a step toward, but still a long way from, adopting the changes in social policy that are necessary to improve the standard of living and quality of life of Americans. Until such changes occur, health care costs will continue to rise and the health of the nation will remain poor in contrast to the rest of the developed world.
There is substantial evidence that children’s health is directly correlated with income and inequities in access to resources and services. The American Academy of Pediatrics has called for an effort to reduce childhood poverty and to mitigate the adverse outcomes of challenging social circumstances in order to obtain and maintain good health.
Many indicators on kidsdata.org describe social determinants of health, the family and community factors that affect individuals’ health and well being. Social determinants can help make individuals’ health better or worse. Examples include economic well being, housing stability, community connectedness, and parents’ physical and mental health.
Healthy People 2020—Social Determinants of Health
Poverty and Child Health
Beyond Health Care: The Role of Social Determinants in Promoting Health and Health Equity
Posted by kidsdata.org
Post Comment


